

Hire Aligned Physicians with Less Chasing
and fewer late stage surprises
Fewer wasted interviews and fewer surprises later. Tessellate helps hiring teams understand how physicians evaluate roles by turning market insight into measurable hiring decisions.
Not a job board or recruiting agency.


What Tessellate is
The bottleneck is not access to more physician profiles. The bottleneck is decision clarity.
Job boards sell visibility. Agencies sell access. Tessellate is built around fit, intent, and measurable hiring signal. Your team sees interest only after a physician has reviewed the role, understood the realities, and opted in.
Physician-led intros
Interest with context — not cold outreach
Engage only after opt-in
No profile blasting
Pre-aligned from the start
Fast Pass packets
Clarity before the first conversation
Verfiied must-haves upfront
Context that drives better conversations
Fewer resets, higher conversion
Hiring intelligence
A system for improving hiring
Diagnose breakdowns in your funnel
Benchmark against real alternatives
Act with precision
Physicians control identity + sharing. Employers only see aggregated unit insights until a physician opts into an intro.
How hiring decisions become clearer
Step 1

Anonymous alignment
Physicians explore fit privately, without pressure or exposure.
Step 2
Questions answered
(still anonymous)
Role-specific realities are clarified early so expectations match reality on both sides.
Step 3
Consent to connect
Only physicians who see a clear fit opt in to introductions - filtering out late-stage drop-off.
Step 4
Fast Pass introduction
Hiring teams receive decision-ready context, not raw interest.


Built for in-house teams and leader-led hiring
We have a recruiting team
(Press the switch)
We don’t have a recruiting team
(Press the switch)
With in‑house recruiters
(Co‑pilot mode)
Physician‑approved intros that meet your requirements—qualified, interested, ready to interview.
We pre‑fill forms; recruiters review & attest—less rework.
One thread through email (ATS APIs coming); higher show‑rates.
Signal reporting: early “why not” so reqs can be tuned
No in‑house recruiters
(Full‑service mode)
We act as your on‑call recruiting desk—no ATS required.
You define the role once (12‑min unit survey); we run the search.
We assemble documents, coordinate interviews, and keep everyone updated.
You decide only on who to meet and who to hire.
Works with or without an ATS
HIPAA‑aligned; zero PHI required
No placement fees


Your fast pass packet
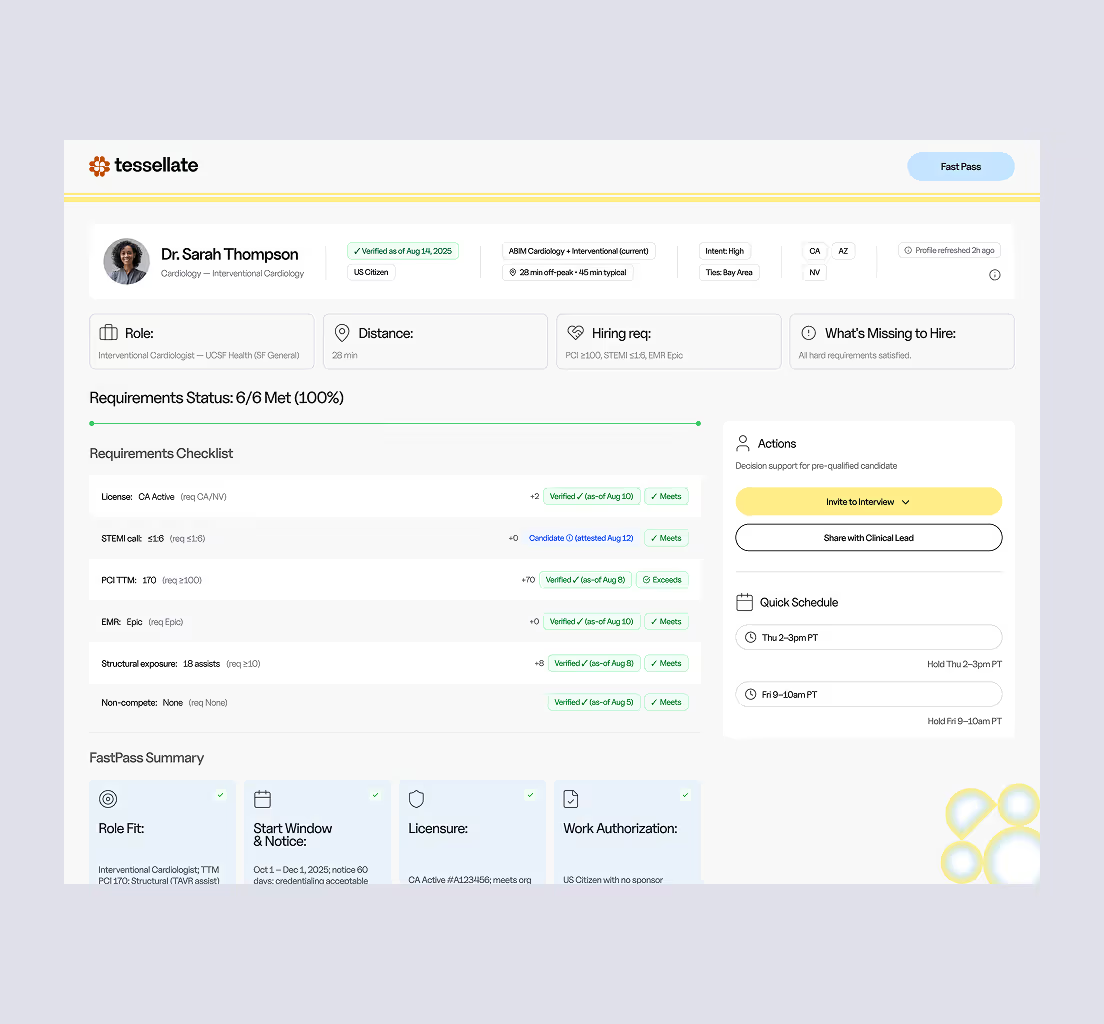
Fast Pass introductions start with decision clarity
A standardized, decision-ready view so first conversations are productive.
Standardized application
Fully pre-filled from physician intake; exportable fields.
Fit reasons
Top “why this matches” mapped to Clinical / Lifestyle / Financial / Location.
Physician attestation
Candidate affirms accuracy before the intro.
Scheduling windows
Two or three time options; we coordinate calendars and send ICS invites.
Gaps to verify
The 2-3 items that merit discussion early.
Credentials
Licenses, DEA/CSR, board cert, NPI, CV
Signal trail
What the physician is solving for; reasons for “yes/no”; follow-ups.
Less chasing, more interviewing
Today’s reality
Repeated re-screening
Key questions answered late
Fragmented information
Scheduling friction
Consent-based intro
You start with interest confirmed.
Packet-complete
Fewer form gaps and rescreens.
Scheduling relay
Interviews confirmed faster, with higher show-rates.
Signal reporting
“Why not” is captured early so reqs can be tuned.
Insights & benchmarks
Powered by physician signals and medical leaders
We show what physicians are solving for—and how your roles stack up—using preference data across up to 130 criteria and anonymized inputs from clinical leaders. Use the benchmarks now, and add your realities to sharpen them.
What you get
Acceptance drivers (by specialty & setting)
What moves physicians to interview and accept: schedule/call mix, comp ranges, autonomy, team makeup, location constraints.
Funnel & speed
Time‑to‑first‑interview, interview→offer conversion, most common decline reasons.
Competitive position (aggregate)
Where your offer lands relative to market expectations—without naming organizations.
Signal trail
The “why” behind physician yes/no so you can tune reqs early.
Contribute: medical leader survey
Why contribute
Calibrate benchmarks to your reality; shorten rework; help your service line win more acceptances.
What we ask
Care settings, call structure, autonomy, staffing mix, must‑haves/flex.
What you get back
Quarterly aggregates and a brief on your specialty/market.
Cross-specialty
(National)
Interview speed wins: +31% acceptance when the first interview ≤ 7 days.
Why: Momentum reduces parallel shopping and drop-off.
IM Outpatient
(Southeast)
Role tuning works (call + hybrid).
After moving call 1:4 → 1:5 and adding 1 remote day/week: pipeline +38%, time‑to‑first‑interview –19% within 30 days.
Why: Small, published changes unlock aligned candidates fast.
Emergency Medicine
(Great Lakes region)
Single-coverage nights deter.
Acceptance −26% where single-coverage nights and annual volume >45k; adding float coverage restores +14%.
Why: Safety staffing is a first-order screen.
Hospitalist
(National)
Admit cap is decisive.
+41% approve‑intro rate when admit cap ≤12/day is stated; –23% when cap is >18/day or unstated.
Why: Workload clarity drives early engagement.
Every place physicians practice
If you employ or contract MD/DOs for clinical care
in the U.S., you’re in scope—large or small, public or private. We partner with health systems and independent groups.
Methods: how we count
Independent medical groups & private practices
Single‑specialty (e.g., ortho, GI, cardiology, psych, EM, HM, anesthesia, radiology, pathology), multi‑specialty groups, physician‑owned practices, MSO/PE‑backed platforms.
Outpatient & procedural sites
Hospital‑owned clinics, independent clinics, ASCs, urgent care, employer on/near‑site clinics, retail clinics where physicians practice, RHCs.
Health systems & hospitals
Academic medical centers, community hospitals, children’s hospitals, critical access hospitals, specialty institutes.
Community & public
FQHCs/CHCs, county/city clinics, VA/DoD/MTFs, IHS, correctional health.
Telehealth & hybrid groups
Virtual‑first or mixed models where physicians deliver care.
Academic departments with clinical appointments
Faculty practice plans and subspecialty divisions.
FAQ: How Tessellate works
What is Tessellate (and what isn't it)?
Tessellate helps physicians explore new roles privately, intelligently, and without recruiter pressure. Behind the scenes, we look at how physicians actually experience roles day to day – be it scope, autonomy, incentives, or expectations – so that introductions are based on fit, not volume.
Tessellate is not a job board, not a resume database, and not a contingency recruiting firm. There’s no spam, no blind submissions, and no pressure to move before you’re ready.
Every introduction happens only with physician consent, and only when there’s a clear case for mutual fit.
What makes Tessellate different from traditional sources?
Traditional recruiting sources optimize for volume; Tessellate optimizes for decision quality. Instead of pushing roles based on availability or urgency, we surface opportunities based on measurable details about how a role actually functions, so physicians can assess fit before investing time or energy.
How does Tessellate ensure alignment with our needs?
Most matching breaks down because it relies on titles and keywords. Tessellate focuses on how a role actually functions.
By grounding each match in clinical scope, working conditions, and real expectations, we make it easier to see where fit is strong and where it needs validation, so teams spend time on the right conversations.
How does the process work?
Physicians explore roles privately and without pressure. You’re only engaged when interest is mutual.
We then provide a Fast Pass and Unit Snapshot that surface what matters most, so teams can quickly assess fit before investing time.
How quickly will we see matched candidates?
There’s no fixed timeline, but clarity drives speed.
Teams that articulate scope, working conditions, and priorities up front and respond promptly tend to see stronger interest sooner.
Do you replace our recruiters or ATS?
No. Tessellate complements your existing recruiters and systems by reducing clutter and improving decision quality.
Your team remains in full control of interviews and offers, and you can start without any ATS integration.
What if we don’t hire someone through Tessellate right away?
That’s okay. Tessellate is built to improve clarity, not rush decisions.
Even without an immediate hire, teams gain a clearer understanding of how their role is perceived and what may need refinement, leading to better conversations and stronger outcomes over time.
How do you protect our data and physician privacy?
Physicians remain anonymous unless they choose to engage, and recruiter outreach is not permitted.
Employer data is used only to support your hiring efforts, with any broader insights shared in aggregate and without identifying individual teams.







